The impact of ammonia on autism: A neurotoxin that affects brain development
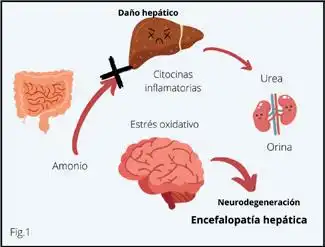
Ammonium is a potent neurotoxin that has a negative impact on neurodevelopment. It is a nitrogen-containing compound produced by protein catabolism. Ammonium is produced in large quantities in the small intestine by the deamination of glutamine and under normal conditions is processed and eliminated by the liver in the form of urea, which is then excreted in the urine. Altered levels of ammonium are associated with metabolic dysfunctions and an unbalanced microbiota.
Three-dimensional representation of the ammonium molecule
Every day, an individual consuming a high-protein diet produces about 1,000 mmol of NH4+; this amount includes NH4+ that comes from food metabolism (exogenous proteins) and from the catabolism of the body, especially of muscle (endogenous protein).
A small fraction of ammonium is used in the synthesis of proteins, creatinine, polyamines, arginine, nucleotides and other essential compounds; while the excess, being neurotoxic, must be eliminated quickly and efficiently from the body. It is mainly eliminated through the urea cycle, which takes place in the periportal hepatocytes. The remaining ammonium is eliminated by the action of the enzyme glutamine synthetase, located in the perivenous hepatocytes, which binds an ammonium molecule to glutamate to form glutamine.
The problem arises when the body cannot eliminate ammonium efficiently, it accumulates in the blood, which is known as hyperammonemiaThis excess of ammonia in the blood has harmful effects on the brain, as it affects the function of brain cells, altering neurotransmission and normal brain development.
In different research papers, researchers found that children with ASD have higher levels of ammonia in the brain and blood compared to neurotypical children. This excess ammonia appears to interfere with neural connections, which could contribute to the cognitive and behavioral difficulties seen in autism.
Chronic exposure to ammonia may alter brain plasticity, that is, the brain's ability to adapt and learn from new experiences, which has direct implications for the cognitive and emotional development of children with autism.
How does ammonia affect the brain?
Its effects include:
Disturbance of neurotransmitter balance: Ammonia can affect the synthesis and release of key neurotransmitters such as glutamate and GABA, which are essential for regulating behavior and learning.
Oxidative stress and neuroinflammation: Ammonia accumulation can generate free radicals and activate microglia, promoting chronic brain inflammation, a common finding in children with ASD.
Mitochondrial dysfunction: Ammonia has been documented to affect the function of mitochondria, the “energy factories” of cells, which could exacerbate metabolic problems present in some children with ASD.
Mild cerebral edema: At higher levels, ammonium can cause a buildup of water in the brain, affecting osmotic balance and neuronal function.
Ammonia-producing bacteria and factors that promote their proliferation
Humans are born in a completely sterile state and begin to acquire their microbiota immediately after birth, mainly through the mother and the initial environmental environment. The term microbiota refers to the community of living microorganisms (bacteria, fungi, viruses, archaea and protozoa) gathered in a specific ecological niche such as the intestine, skin, mouth, or any other part of the body; the microbiome includes both the microorganisms that make up the microbiota and their genetic material (genomes), metabolites and functional interactions in the environment they occupy.
The gut microbiome is a key component in ammonium production. Ammonium-producing bacteria play an important role in intestinal metabolism, these bacteria generate ammonium mainly through the activity of the enzyme urease, which breaks down urea into carbon dioxide and ammonium. Among the most relevant bacteria in this process are those of the genus:
1. Proteus, contributes significantly to the accumulation of ammonia in the intestines and in circulation.
2. Klebsiella, associated with intestinal dysbiosis and metabolic disorders, especially in people with liver and neurological problems.
3. Helicobacter pylori, known for its role in gastric ulcers, produces large amounts of ammonia to neutralize gastric acid, creating a favorable environment for its survival.
4. Escherichia, some strains of Escherichia coli They have ureolytic capacity and can contribute to the production of ammonium, especially in situations of bacterial overgrowth.
5. Clostridium, some species of Clostridium They can also produce ammonium as a byproduct of amino acid fermentation, which exacerbates the accumulation of toxic metabolites under conditions of dysbiosis.
6. Methanogenic bacteriaAlthough they do not directly produce ammonium, they facilitate the metabolism of nitrogenous compounds that can release ammonium as a byproduct.
The factors that favor the proliferation of these bacteria are:
1. High protein diets, which increases the availability of urea and amino acids, ideal substrates for these bacteria.
2. Intestinal dysbiosis, the loss of balance in the microbiota allows these bacteria to grow uncontrollably.
3. Specific intestinal conditions, such as SIBO, leaky gut syndrome, and liver disease, which make it difficult to efficiently eliminate ammonia.
Mild or moderate hyperammonemia in children with ASD
Hyperammonemia, characterized by elevated blood ammonia levels, is a condition known primarily for its severe manifestations in rare metabolic diseases.
According to research, children with ASD may present mild or moderate levels of hyperammonemia, which could be due to a congenital error of metabolism that causes organic acidemia, defects in the oxidation of fatty acids and hyperinsulinism syndrome; due to defects in the enzymes that catalyze the urea and arginase cycle, in addition to failure in the intermediary transport of the urea cycle; as well as due to bacterial overgrowth that generates a deregulation in the symbiosis of the intestinal microbiota (IM) causing dysbiosis in the patient (Moreno & Garcés, 2022).
However, it is important to clarify that there may be various situations where hyperammonemia does not correspond to a metabolic disorder, such as exposure to certain medications, parenteral nutrition, or liver failure, and these should be taken into account for differential diagnosis.
Possible causes of hyperammonemia in ASD are:
1.Genetic mutations Deficiencies in urea cycle enzymes can lead to a reduced ability to remove ammonium.
2. Intestinal dysbiosis increases the production of ammonium from the fermentation of proteins in the intestine.
3. High protein diet overloads protein metabolism, especially if there are underlying enzyme deficiencies.
4.Liver or intestinal dysfunction may limit the ability to process and eliminate ammonium.
Hyperammonemia causes cerebral edema, disrupts synapses, and induces neuronal and glial cell death. The developing brain is more susceptible to damage from hyperammonemia, although in older individuals in whom the cranial sutures are already closed, cerebral edema may have more serious consequences such as brain herniation.
In the event of an episode of hyperammonemia, the priority is to protect life and safeguard the integrity of the central nervous system by reducing blood ammonia levels to normal values through urgent medical treatment, life support and individualized nutrition.
Types of hyperammonemia
According to the cause of hyperammonemia, and these are classified into primaries and secondary according to their origin:
1. Primary hyperammonemia
It is due to genetic defects in the urea cycle, which is responsible for removing ammonia from the body. These conditions usually manifest in early childhood and can have a significant impact on neurological development. Some examples include:
Ornithine transcarbamylase deficiency (OTC): One of the most common urea cycle disorders, which can cause severe neurological symptoms if left untreated.
Argininosuccinate synthetase or argininosuccinate lyase deficiency: Associated with accumulation of ammonia and other toxic substances that affect the brain.
In children with autism, genetic alterations in the urea cycle could contribute to increased plasma ammonia and exacerbate ASD symptoms.
2. Secondary hyperammonemia
This type arises due to external factors or metabolic diseases that indirectly affect the elimination of ammonia. The most common causes include: SIBO, intestinal dysbiosis, high protein diets or excessive supplementation, liver disease or medications such as valproic acid used to treat epilepsy in children with ASD, can cause hyperammonemia as a side effect.
Warning signs and symptoms
Symptoms result from neurotoxicity caused by ammonia and may vary depending on age and the type of enzyme defect present. The main clinical manifestations of hyperammonemia include:
Ammonium level 100-200 µmol/L
Vomit
Hyporexia
Food refusal
Irritability
Gait disturbance
Slow reaction to verbal stimulus
Dysarthria
Sleepiness
Lethargy
Clinical picture similar to sepsis
Ammonium level 200-400 µmol/L
Dizziness
Mental confusion
Obnubilation
Behavioral disturbance
Disorientation
Slow reaction to physical stimulus
Ataxia
Agitation
Hallucinations
Psychiatric symptoms
Seizures
Shortness of breath (hyperventilation)
Hypo/Hyperthermia
Loss of vision
Ammonium level > 400 µmol/L
Apne
Cerebral edema
Liver failure
Circulatory failure
Coma
Multiple organ failure
Ammonium level >1000 µmol/L
Decortication
Brain death
Diagnosis of hyperammonemia
Blood test
The main method for diagnosing hyperammonemia is by blood tests, ideally fasting and under controlled conditions, which measure plasma ammonia levels. Elevated blood ammonia levels confirm the diagnosis. It is essential to perform the sample collection with the patient as calm as possible and, if possible, avoid crying, since muscle tension and the use of tourniquets can raise values by 10-15%. This increase occurs due to the release of ammonia by erythrocytes and the deamination of amino acids, especially glutamine.
Genetic testing
Genetic testing can evaluate defects in the urea cycle, identify specific enzyme deficiencies, and confirm the diagnosis.
In addition, it may be necessary to assess:
Liver function.
Organic acids in urine to rule out metabolic errors.
Gut microbiome profile.
Treatment of hyperammonemia
Understanding the medications and methods available to remove ammonia, as well as the energy, protein, supplement, cofactor and vitamin needs, is essential to making appropriate medical and nutritional decisions, considering the clinical, biochemical and underlying disease condition of each patient.
Therefore, the pharmacological management of hyperammonemia must be individualized according to the etiology, the patient's general condition, ammonia levels and availability of medications. Management includes dietary strategies, supplements and medical treatments:
Dietary strategy:
Reduce excessive protein intake while ensuring adequate supply for growth.
Probiotics and prebiotics that help balance the microbiome and reduce intestinal ammonia production
Supplements and medications:
2.1. Ammonium production reducing agents
2.1.1. Non-absorbable disaccharides
Lactulose and lactitol: Lactulose, also known as 1,4 ß galactoside-fructose, is a synthetic disaccharide composed of galactose and fructose. Lactitol is also a disaccharide, composed of galactose and sorbitol.
Polyethylene glycol (PEG): PEG is a polymer that is not absorbed by the gastrointestinal tract, characterized by its biocompatibility, amphiphilicity (ability to be hydrophilic and hydrophobic at the same time) and high hydration capacity. Due to these properties, it acts as a very effective osmotic laxative.
2.1.2. Antibiotic
Neomycin: Antibiotic from the aminoglycoside family, broad spectrum with low absorption at the systemic level (3-5%), its main action is to reduce the bacterial load at the intestinal level, with the consequent decrease in the production of ammonia and nitrogenous substances.
Rifaximin: Non-absorbable drug, since only less than 1% of the administered dose can be detected in blood. It has specific activity at the intestinal level, functioning as a broad-spectrum antibiotic that decreases the activity of bacterial endotoxins at the intestinal level, decreasing the production of ammonia.
2.1.3. Sodium phenylbutyrate: EIt is a prodrug that is transformed into sodium phenylacetate, when combined with glutamine, it forms phenylacetylglutamine, achieving the urinary elimination of 2 moles of nitrogen for each mole of phenylbutyrate.
2.2. Agents that increase ammonium removal
2.2.1. Carglumic acid: Carglumic acid or N-carbamylglutamate has proven very useful in rapidly decreasing ammonia levels and reducing episodes of hyperammonemia.
2.2.2. L-arginine and L-citrulline: Citrulline is a precursor of arginine, which when hydrolyzed forms urea and ornithine, necessary to restart the urea cycle. Arginine is therefore supplemented as such or as its precursor L-citrulline, to maximize ammonium excretion, activating the urea cycle.
2.3. Other useful medications for hyperammonemia
2.3.1. Levo-carnitine (L-carnitine): It transports long-chain fatty acids, modulates intracellular CoA homeostasis, regulates mitochondrial enzyme activity, improves insulin resistance, and has antioxidant and anti-inflammatory properties.
2.3.2. Biotin and hydroxycobalamin: Known as vitamin H, an essential nutrient for the body: it helps in the conversion of food into energy, the formation of proteins and the functioning of the nervous system.
At Enevia we offer specialized consulting services and different tests that can guide you in different areas such as neurology, genetics, nutrition and general medicine, as well as help you make the right decisions and analyze medical tests to achieve effective treatment for the pathologies that you may suffer from.
Article written by Enevia Health Advisor and Collaborator:
Yohana Cespedes, Chemical Eng.
Bibliography
Carrillo R, Noriega M, Sánchez R. Ammonia and hyperammonemia. Its clinical significance. Journal of Medical Research Sur 2008 Jul; 15 (3).
Guarner F. Intestinal microbiota and inflammatory bowel diseases. Rev. Gastroenterol Hepatol. 2011 March; 34(3):147-154
Häberle J. Clinical and biochemical aspects of primary and secondary hyperammonemic disorders. Arch Biochem Biophys. 2013 Aug 15;536(2):101-8. doi: 10.1016/j.abb.2013.04.009. Epub 2013 Apr 27. PMID: 23628343.
Kido J, Matsumoto S, Ito T, Hirose S, Fukui K, Kojima-Ishii K, Mushimoto Y, Yoshida S, Ishige M, Sakai N, Nakamura K. Physical, cognitive, and social status of patients with urea cycle disorders in Japan. Molecular Genetics and Metabolism Reports 2021 Jun (27).
López-Mejía L, Revilla N, Guillén-López S, Carrillo-Nieto I, Fernández Lainez C, Ibarra González I, Vela Amieva M, Belmont Martínez L. Neurobehavioral alterations in children with autism associated with level of plasma ammonia and urea hydrolizyng bacteria. Acta Pediatr Méx 2022; 43 (5): 293-313.Ribas GS, Lopes FF, Deon M, Vargas CR. Hyperammonemia in Inherited Metabolic Diseases. Cell Mol Neurobiol. Nov 2022; 42(8):2593-2610. DOI: 10.1007/s10571-021-01156-6. Epub Oct 19, 2021. PMID: 34665389.
We use cookies to optimize our website and our service.
Functional
Always active
The storage or technical access is strictly necessary for the legitimate purpose of allowing the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication through an electronic communications network. .
preferences
The storage or technical access is necessary for the legitimate purpose of storing preferences not requested by the subscriber or user.
Statistics
Storage or technical access that is used exclusively for statistical purposes.Storage or technical access that is used exclusively for anonymous statistical purposes. Without a requirement, voluntary compliance by your Internet Service Provider, or additional records from a third party, information stored or retrieved solely for this purpose cannot be used to identify you.
Statistical
Storage or technical access is necessary to create user profiles to deliver advertising, or to track the user across one or multiple websites for similar marketing purposes.
Our groups are the ideal platform to learn and share your scientific concerns about neurodevelopment issues
Group rules:
Be nice. Bullying, insults and personal confrontations are not allowed.
Respect everyone's privacy.
Use information that is as scientific and reliable as possible, cite sources.
We want to comply with WhatsApp rules and avoid topics that we know lead to the closure of groups, so we ask that these groups not discuss topics related to VACCINES, MMS, CDS.
*Our purpose is informational only, it is not intended to be a substitute for medical advice, diagnosis or treatment.